

Background: Venetoclax (Ven)-based regimens are highly effective in treating patients with chronic lymphocytic leukemia (CLL), effecting clearance of detectable minimal residual disease (MRD) in many patients after just 1 year of therapy. Approximately, 30% of patients fail to clear detectable MRD within this time period and risk developing, progressive disease (PD) despite continued Ven therapy. Moreover, these patients have a relatively short progression free survival (PFS) after stopping fixed-duration therapy. Therefore, development of consolidation strategies to eradicate detectable MRD and/or to mitigate the risk of PD in patients who fail to clear MRD after 1 year of Ven-based therapy is of vital clinical importance.
In particular, patients who fail to clear MRD after 1 year of Ven-based therapy harbor CLL cells with high-level expression of ROR1, an oncoembryonic protein expressed by a broad array of incurable malignancies. Patients who are refractory to MRD-clearance on Ven-based therapies have gene-expression signatures reflective of high-level ROR1-signaling, which can be inhibited by the anti-ROR1 mAb, Cirmtuzumab (Choi et al., Cell Stem Cell. 2018; 22: 951-959). Prior studies demonstrated that Cirmtuzumab and Ven have at least additive activity in promoting cytotoxicity of CLL cells in vitro (Rassenti et al. PNAS. 2017;114(40):10731-10736). As such, cirmtuzumab may be an effective consolidation strategy for patients who fail to clear MRD following completing 1 year of Ven-based therapy.
Study Design and Methods:
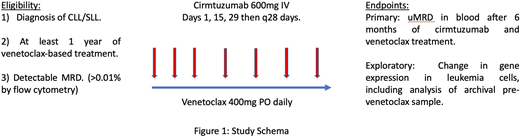
Study Design: We initiated a single center, phase 2 Simon's two-stage-designed study to determine the efficacy of Cirmtuzumab plus Ven combination therapy in patients who fail to clear detectable MRD (defined as > 0.01% of the blood mononuclear cells, as assessed by flow cytometry) after ≥1 year of Ven-based therapy (NCT04501939). Enrolled patients will receive cirmtuzumab at 600 mg IV, q14 days for 2 doses and then monthly thereafter. Patients will continue oral Ven at 400mg daily and be monitored for safety and PD. Following 6 months of Cirmtuzumab + Ven, patients will be assessed for MRD in the blood. At the discretion of the treating physician, patients may continue combination treatment for up to one year (Figure 1).
Major Eligibility Criteria: Patients must have a diagnosis of CLL with detectable MRD after having received ≥ 12 months of Ven-based treatment . Patients will be excluded from the study if they have an uncontrolled medical co-morbidity, which compromises their capacity to complete the study, or if they are receiving treatment for CLL with agents other than Ven.
End Points: The primary end-point of the proposed study is clearance of detectable MRD in the blood after 6 months of cirmtuzumab + Ven therapy. Secondary end-points include safety and time to next CLL treatment. Exploratory end-points include changes in gene expression in leukemia cells, including analysis of archival pre-Ven treatment samples, when available.
Statistical Methods: We used a Simon's two-stage minimax design at 5% significance level to test the scientific hypothesis that 6 cycles of cirmtuzumab + Ven will achieve undetectable MRD (a 'response') in more than 5% of patients, against the null hypothesis of less than a 5% response rate. In the first stage, we plan to accrue 12 patients. If none of these patients respond at 6 months, the study will close. Otherwise, we will accrue an additional 4 patients for a total of 16 patients. If three or more patients respond, the primary endpoint of the trial will have been met, demonstrating an MRD clearance rate greater than 5%. The trial is designed to have 80% power to provide such evidence at the 5% significance level if the true rate of clearance of MRD is 25% or greater.
Heyman:Oncternal Therapeutics, INC: Research Funding. Choi:Pharmacyclics/Abbvie: Research Funding; Genentech: Consultancy. Jamieson:Forty Seven Inc: Patents & Royalties; Bristol-Myers Squibb: Other. Kipps:Genentech/Roche: Membership on an entity's Board of Directors or advisory committees, Speakers Bureau; VelosBio: Research Funding; Oncternal Therapeutics, Inc.: Other: Cirmtuzumab was developed by Thomas J. Kipps in the Thomas J. Kipps laboratory and licensed by the University of California to Oncternal Therapeutics, Inc., which provided stock options and research funding to the Thomas J. Kipps laboratory, Research Funding; Celgene: Honoraria, Research Funding; Ascerta/AstraZeneca, Celgene, Genentech/F. Hoffmann-La Roche, Gilead, Janssen, Loxo Oncology, Octernal Therapeutics, Pharmacyclics/AbbVie, TG Therapeutics, VelosBio, and Verastem: Membership on an entity's Board of Directors or advisory committees; Gilead: Membership on an entity's Board of Directors or advisory committees, Speakers Bureau; Pharmacyclics/ AbbVie, Breast Cancer Research Foundation, MD Anderson Cancer Center, Oncternal Therapeutics, Inc., Specialized Center of Research (SCOR) - The Leukemia and Lymphoma Society (LLS), California Institute for Regenerative Medicine (CIRM): Membership on an entity's Board of Directors or advisory committees, Research Funding, Speakers Bureau.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal